

|
|
1.INTRODUCTION1.1MenorrhagiaMenorrhagia is technically defined as menses lasting longer than 7 days or blood loss volume in excess of 60-80 ml per menstrual cycle. The bleeding is secondary to imbalanced secretions of pituitary and ovarian hormones leading to erratic and abnormal endometrial responses that culminate in hemorrhage (1). It is one of the common problems in gynecology, although half of the cases show no underlying pathology and no specific etiology. Some patients have as high as a 400 ml loss of blood per menstrual period (2, 3) which can result in iron-deficiency anemia (1). Abnormal uterine bleeding has been a common problem for women throughout the world, although the choices for women are limited: hysterectomy or removal of the uterus, medical treatment that induces a peri-menopausal state, or living with the discomfort. Hysterectomy procedures are costly, have a long hospital stay and a very long recovery period for the patient before return to normal activities. Average hospital stay for a vaginal hysterectomy is 7.4 days and for abdominal hysterectomy is 9.0 days. In addition, hysterectomies cost health insurers $1.7BB/year in the US. Any alternative procedure that will reduce the medical and economic toll is desirable, especially if it preserves the uterus (4). Historically, alternate treatments given for ablation were often uncontrolled and included superheated steam, cryotherapy, urea injection, cyanoacrylate, and radium packing. In spite of this varied and highly experimental work, no safe method prevailed (5). 1.2Recent alternatives to hysterectomyThe bleeding originates in the endometrium, the inner layer of the uterus. If proper transcervical access is attained using small endoscopes (hysteroscopes), the endometrium becomes accessible for treatment. A recent surgical treatment performed under video guidance has been to apply radiofrequency (RF) energy to a rolling ball or barrel for ablation of the endometrium. By ablating the endometrium, it is possible to stop or at least reduce the bleeding so that women can lead a more normal life. Unfortunately, the complex geometry of the endometrial surface combined with the lack of assessment of deep thermal damage with only superficial observation in a 2-D scope system, make rollerball ablation dependent on the skill of the user. Each menstrual cycle, the endometrium regenerates and is then progressively sloughed. Endometrial ablation is the destruction of the inner lining of the uterus with heat, cold, resection, or vaporization in order to lessen the activity of this layer and reduce bleeding. Pre-menopausal women are typically candidates for this procedure, although post-menopausal women on hormone replacement therapy are also showing interest. About 22 percent of women in the US have excessive menstrual bleeding which translates into a group of 7.6 million women, and the amount of bleeding can cause severe anemia. Most women prefer to retain their uterus, as seen in the reduction in the number of hysterectomies in the US by about 100,000 in last 20 years. In addition, the medical training programs are graduating more women gynecologists who may have quite a different attitude towards hysterectomy. Even subtotal hysterectomies that do not remove the ovaries have drawbacks and can bring on early menopause. An additional function of the uterus and its ligaments is to support other abdominal organs and help maintain lubrication of the cervix, which is important for normal sexual function. The ideal technique to treat abnormal bleeding will utilize minimally invasive techniques. A major surgery will thus be replaced by an ablation treatment performed in the office, with minimal discomfort to the patient during and following treatment. Several available ablation methods are being developed that make this treatment simple to administer and receive. Several of the treatments are done under the supervision of a computer such that the quality of the heat treatment is carefully monitored and controlled, to parameters of time and temperature that are have been shown to be effective in clinical trials. To obviate the need of a surgical procedure and an operating room with general anesthesia, several techniques have been attempted to thermally treat the endometrium. In the early days of using either the Nd:YAG laser or electrosurgical resectoscope, the endometrial layer of the uterus was denuded and underlying basil layer ablated. The arteries were then sealed, preventing regeneration and functioning of the endometrium. As a result of early studies, endometrial ablation is now considered a safe alternative to hysterectomy for management of menorrhagia or abnormal bleeding, especially in cases that have failed to respond to conventional therapy. The popularity of endometrial ablation over hysterectomy has been growing. There has been an exponential increase in the number of surgical endometrial ablation cases in the UK over the period from 1988-1993. In a group of patients surveyed, the main reasons for seeking out an alternative treatment were avoidance of a major surgical procedure, fast recovery and return to normal activity, and short hospitalization (6). Cultural factors also may relate to the number of hysterectomies performed. Fraser et al. (7) found that twenty-five percent of women in New Zealand have hysterectomies. It has been speculated that in a managed care environment, substantial savings can be accomplished by converting to surgical endometrial ablation from hysterectomy. The savings per case would be about $4300. The average cost for hysterectomy is $9222 and for endometrial ablation is $4927, using surgical techniques. The recovery from hysterectomy is 3-6 weeks for the patient and for ablation is one day. If balloon techniques are used instead of surgical ablation, the cost is in the $2500 to $3000 range and return to normal activity is also one day. 1.3Numerical simulation studiesRecently, there have been several technologies applied to the endometrium by applying heat treatments for thermal ablation in an office-based procedure that does not require surgery. These treatments utilize either a hot, fluid-filled balloon for conductive heating or RF patches on the outside of an air-filled balloon to make contact with the endometrial wall. The latter applies RF energy and deposits power in the superficial layers of the endometrium. Still other techniques use microwaves or cryotherapy to treat the endometrium. The target depth of ablation is approximately 5 mm. Due to the wide variety of parameters that effect heating, a finite element model was created to predict temperature distributions in the uterus. Some of the parameters studied include blood flow, type of heat source, heat source temperature, heat application time, blood vessel presence, and temperature-dependent, electrical properties and perfusion. The paper will develop two numerical models for a conductive and an RF heating system for treatment of the endometrium based on the bioheat equation (8). Actual devices used clinically will be modeled with temperature set points used. Lesions produced by RF ablation are heat induced and depend on the temperature distribution resulting from the electric field in the tissue. Unlike earlier work in the hyperthermia range of 40-55°C for adjuvant therapy (9, 10, 11) target temperature for thermal ablation is in the range of 60-110°C, where tissue desiccates and thermal and electrical properties change substantially (12). Values of electrical conductivity with changing temperatures for tissues excited at 500 kHz were not available, thus measurements of electrical conductivity over time at various temperatures were made as input to the model (12). This was more accurate than assuming that temperature-induced changes in conductivity were 2%/°C (13), up to 100°C (14). Changes to thermal conductivity were also measured as input to the model (Roop Mahajan, personal communication). The tissue perfusion term is rate of mass flow of blood per unit mass of tissue. Flow is considered to occur at the capillary level and due to the convoluted nature of capillary beds, causes it to be non-directional (15). Blood perfusion is also a temperature dependent function that can be rescaled due to tissue reaction to heating which will initially increase flow in normal, but not in pathologic tissue; and then proceed to decrease due to desiccation and capillary shutdown, and finally, blood coagulation at 60°C (12). 2.CLINICAL STUDIES2.1Loop resection during surgeryAs an early alternative to hysterectomy, a surgical procedure was done inside the uterus under direct visualization. This procedure used a small diameter rigid endoscope called a hysteroscope, as well as an electrosurgical loop to resect the endometrium and part of the myometrium. Typically, endometrial ablation was done in a patient population of 35-45 year old women that were premenopausal. Brooks and Serden (16) performed a study in a group of 26 patients, ages ranging from 50 to71 years (mean 54). All patients underwent hormone replacement therapy prior to endometrial ablation. An 8 mm diameter loop electrode was used to shave the endometrium to a depth of 3-4 mm using 110 W in cut mode. The surface was then coagulated with a rollerbarrel or rollerball electrode at 80-90 W blend mode. A study of 500 patients by Nicholson et al. (17) performed endometrial resection. Complications that resulted were 2.4% uterine perforation and one patient with electrosurgery injury to the small intestine. In the group, 19% had a hysterectomy performed sometime after the resection. Experience was a factor since a higher success rate correlated to greater than 10 procedures done by the surgeon. The 5 year results showed a 62% success rate and a 21% hysterectomy rate. 2.2Rollerball ablation during surgeryPredating the above studies, a study by Vancaillie (18) demonstrated early work to provide techniques for endometrial ablation. Prior to endoscopic development for the uterus, a urologic resectoscope was used. A rolling electrode termed “rollerball” was passed over tissue with RF electrocautery activated. The requirement in rollerball ablation was that thermal damage had to cover the entire endometrium, deep enough to destroy the basil layer. The ball was 2 mm in diameter and a power level of 40-70W in coagulation mode was used. The ball had a 4 mm2 surface area in contact with tissue and was moved at a rate of 10 mm/s. The study emphasized that with a ball electrode, it would be difficult to cut through the uterine wall, as when using a loop electrode. The endometrial surface was passed over once with the rollerball during this 15-30 minute ablation procedure. In clinical follow-up, a watery discharge was seen up to 6 weeks. Van Damme (19) also conducted a rollerball ablation study. Rollerball coagulation was done in long, overlapping strips, from the fundus to the internal osteum of the cervical canal. The cervical canal was avoided to prevent stenosis with the risk of hematometria. The rollerball was moved rapidly to achieve hemostasis on the first pass. On the second pass, the rollerball was moved slowly and pressure applied until the smooth layer of endometrium completely disappeared and the irregular layer of crisscrossing muscular fiber was visible. It was found that electrosurgical endometrial ablation resulted in a wide-open uterine cavity, contrasting with Nd:YAG laser ablation, which commonly left a stenotic cervical canal with nearly total obliteration of the cavity by fibrosis (20). To avoid hysterectomy, a treatment involving hormone therapy is often tried first. The measured blood loss in patients undergoing hormone therapy is 95 ml with a 5.6 day average length of period. Following rollerball ablation, the blood loss at one and six months was reduced to 0.4 and 1.0 ml and the duration was 0.2 and 0.9 days, respectively. The patients pre-treated with hormone therapy had a very thin endometrium of 2 mm thickness (7). Fraser et al (21) performed rollerball ablation using an 8 mm resectoscope with 1.5% glycine as irrigant. A coagulation current was used at power levels of 40-100 W. Two rollerball applications were done of the entire endometrium under direct visualization. The procedure took an average of 46 minutes under general anesthesia. Post-operatively, there was an initial period of light red bleeding followed by watery drainage over a 1-5 week period. The incidence of amenorrhea was higher in the study group with higher power (>80 W) than in the 40-70 W group. The volume of blood loss was initially 104 ± 19 ml which reduced to 4.8 ± 2.9 ml at 3 months and to 1.7 ± 1.1 ml at 6 months. Indman and Soderstrom (22) studied the depth of coagulation with the rollerball electrode. A patient underwent rollerball ablation and then had a scheduled hysterectomy four days later. The depth of tissue destruction caused by 19 and 59 W of RF in cut mode was 1.5 and 2.7 mm, respectively. When a coagulation waveform was used at 28 W and 57 W, the depth of damage was 6.1 and 1.8 mm, respectively. Visual effects on the surface do not predict actual tissue destruction, so further in vivo studies will be necessary in order to obtain consistent clinical results. Moseley et al. (23) studied stray RF fields during endometrial ablation procedures in 17 patients. The mean equivalent power density at the position of the surgeon exceeded 10 W/m2. This value was derived from a basic restriction in the average specific absorption rate in the body to 0.4 W/kg, the limit of occupational exposure which is well below that which has been shown to be hazardous to health. Measured values on the field strength suggest that this organ dose limit was not exceeded. It was concluded that staff exposure to stray RF radiation during radio-frequency endometrial ablation is not considered to be hazardous to health. Vercellini et al. (24) compared the cutting loop to a rollerbarrel electrode. The barrel had grooves cut into it for the purpose of concentrating current and increasing the vaporizing effect in tissue (see Lim et al. (69) for an extended discussion). The vaporizing electrode was 3 mm in width and 200 W of RF energy was applied in cut mode. Pressure applied to distend the uterus was 100-120 mm Hg and vacuum suction was -30 to -40 mmHg. One patient had 640 ml fluid deficit in the vaporization group and four had 850 ml deficit in the resection group. Patient satisfaction was 96% in the vaporization group and 93% in the resection group, with amenorrhea rates about the same at 79-80%. On second look laparoscopy, the inner uterine cavern was visually inspected. In the vaporization group, it was shrunken and fibrotic with an endometrium that was either very thin or non-existent. In the resection group, the cavity was tunnel shaped with abolished cornual recesses and also very thin or no endometrium. Patients were pretreated with GnRH agonists which thins the endometrium to 1.0 mm. The depth of furrows for each device was about 3 mm. The mean depth of thermal necrosis was 1.8 mm in the vaporization arm and 0.4 mm in the loop resection arm. The menstrual flow at follow-up was about the same for both groups. 2.3Hot fluid ablationBaggish et al. (25) created a system to treat the endometrium in the office. A saline solution was infused into the uterus without a balloon to thermally treat for 15 minutes. Their initial experimental work was done at 60, 70, or 80°C in the sheep uterine horn and extirpated, human uteri. A small cage was deployed with thermocouples in the fundus to monitor temperatures during treatment. The heater was located in the shaft of the handpiece. During treatment, pressure in the uterine cavity was carefully monitored, since any loss of pressure signaled uterine perforation. In human extirpated uteri, ablations at less than 80°C produced incomplete endometrial destruction at 15-20 minutes duration. The presence of intact endometrial glands and stroma was still seen. If temperatures were elevated in excess of 80°C, endometrial glands were disrupted, stroma collagenized, and no evidence of viability was seen in the superficial myometrium at 1-3 mm depth. Peak serosal temperatures on the outside of the uterus ranged from 35-49°C. During the infusion of fluid, no leakage through the cervix or fallopian tubes was observed, although this was only done on ex-vivo tissue. There is still a possibility of hot fluid leaking into the vagina or into the fallopian tubes and then into the abdominal cavity. 2.4Laser ablationEarly work for endometrial ablation was done with lasers. An Nd:YAG laser was approved by the FDA for use on the endometrium in 1986. Early studies showed deep scattering of the light allowed penetration to 3-5 mm, although if the cavity length exceeded 10 cm, the patients were excluded from the studies because the procedure would take too long (71). All ablations were done under general anesthesia with the uterus filled with saline. Although some studies used a non-contact laser for ablation, this study dragged the laser to create furrows with 40-50 W of power. Contact with the tissue can destroy the fiber tip so a sterile fiber-stripper was kept on the sterile field to do repairs. In the study, 95% of patients ceased menses or had reduced flow (4). Laser probes were applied in a non-contact fashion, with the fiber held 1-2 mm from the tissue, perpendicular to the surface. Contact was made only in the area around the tubal osteum where a light-touch technique created furrows. Following the treatment, a Foley catheter was inserted into the uterus and inflated to tamponade bleeding. The procedure time ranged from 35-180 min. There was a potential for fluid deficit due to the opening of venous channels during laser usage. A pressure of 55 mmHg was required for the tubal osteum to begin to evacuate fluid down the fallopian tubes (4). Donnez et al. (26) used an Nd:YAG laser for transhysteroscopic photocoagulation. Three fibers were inserted and hinged just inside the uterus like an inverted triangle with a length of 3-4 cm. The fibers provided circumferential diffusion and a mirrored coupler split the light among the three fibers. A power of 5-7 W/fiber was used for 300 s. The fiber assembly was easily seen on ultrasound for evaluation of deployment. Ex-vivo uterine experiments showed temperatures of 75 and 47°C, at depths of 0.0 and 10 mm, respectively. At 6-7 mm, which is the target zone, temperatures of 60°C were reached. The maximum temperature measured was 102°C. In the clinical series, one patient at 6 weeks had a disappearance of the endometrium and fibrosis in the myometrium to a depth of 4 mm. A study was done with 86 women with excessive endometrial bleeding by Everett (27). In an outpatient setting, the patients were treated with a sidefire laser. The technique involved blanching the entire anterior and posterior walls with the laser set at 70 W and reflected forward 105°. The ablation took 25-60 minutes and utilized 17-214 kJ of energy. Both energy and time requirement correlated with uterine size. One potential complication whenever a non-physiological fluid is used for uterine distension is fluid uptake by the patient. Eight women had excessive fluid absorption in the range of 700-1500 ml. After 12-72 months following treatment, 82% reported amenorrhea. Fifteen patients (19%) required a single minipad less than 3 days/period. Bleeding requiring 2-3 minipads was experienced in only 1% of the patients. Baggish (28) performed a clinical trial to compare laser and electrocautery. In this clinical series, 401 patients were treated with Nd:YAG laser and 167 with rollerball electrosurgery. Follow-up was done from 1.0 to 4.5 years. In the laser treatments, a 1.0 mm sculpted, fiber-ball was used with a power density of 5000 W/cm2 at power levels of 40-60 W. For the electrocautery arm, a 3.0 mm rollerball was used at a power density of 1700 W/cm2 at power levels of 100-150 W. Either device provided 2-4 mm penetration into the myometrium at these power settings. The success rate was 95% for laser and 87% for electrocautery. In the analysis of amenorrhea, the laser resulted in a rate of 62% and the electrocautery achieved 46%. The total operation took 32.5 min. A group of women that is being given hormone replacement therapy to counteract osteoporosis and other post-menopausal problems, may have abnormal bleeding induced by the therapy. Phillips (29) studied the effectiveness of ablation or resection to control hormone induced bleeding in a group of postmenopausal women aged 47-69 years old. Patients were treated with an Nd:YAG laser for endometrial ablation or an electrosurgical rollerball or a 7 mm wire loop for endomyometrial resection. A total of 93% became amennorheic within 2 months of surgery and remained amenorrheic over the next 8.25 years. High amenorrhea rates suggest that the interoperable bleeding induced by hormone replacement therapy is readily treated by ablation. Although hormone replacement therapy has a positive impact on several organ systems, one undesirable side effect may be excessive or unwanted bleeding. 2.5Conductive heating with balloon devicesBalloon devices brought on the advent of the replacement of a surgical procedure by a computer automated, thermal treatment. The treatment device is inserted into the endometrial cavity and then distended to fill the cavity. To distend the balloon in the uterus, the pressure required was found to be 40 mmHg, within a range of 25-50 mmHg (30). Singer et al. (31) performed a study with a latex balloon inserted into the uterus and filled with 5% dextrose. The intent was to coagulate to a depth of 3-5 mm into the endometrium. In their clinical series, 5/18 patients were anemic from the excessive bleeding, prior to therapy. The balloon was inflated to a pressure of 80 mmHg and heated for 6-9 minutes at 77-88°C. The results were that 83% of the patients had a significant reduction or elimination of bleeding. Neuwirth et al. (32) also studied balloon ablation. A balloon device was fabricated with a heating element inside the balloon and a thermistor on the heater shield in the center of the balloon (33). After transcervical insertion, the balloon was filled with 5% dextrose. The unit sensed pressure and automatically shut down if not in the range of 45-165 mmHg, mainly to protect against uterine perforation. Heat to the fluid was provided by a 12 V DC heater coil. The desired pressure was 70-80 mmHg. The fluid volume injected into the balloon ranged from 5-10 ml and the allowable maximum temperature (Tmax) was set to 92°C. The temperature of the endometrium was measured by placing temperature probes through the myometrium, poking through the endometrium under hysteroscopic guidance, and then withdrawing until the tip was no longer visualized. The Tmax measured was 87-89°C. The study showed that a temperature of 55°C, considered to be the minimum for ablation, never penetrated more than 5 mm into the uterine wall. In a study with the same device (34), the uterine lengths ranged from 5-12 cm. The amount of bleeding was significantly reduced with the thermal treatment. In pads/day, the reduction was from 9.2 (pre-op.) to 3.4 (post-op, follow up). The number of days/cycle was reduced from 9.6 to 4.1 and the number of pads/cycle was reduced from 86 to 19. The amenorrhea rate was 14% and success rate was 89%. A higher balloon pressure (>140 mmHg) correlated to patient success, probably due to the compression of the capillary beds which lead to decreased perfusion. A series of pre-hysterectomy patients was studied with a balloon device. There was no uterine perforation or rupture. The outside uterine wall or serosa rose 1°C during treatment. Histopathology showed that thermal damage was evident as hemorrhage, congestion, edema, eosinophilic infiltration, and necrosis. The mean zone of damage in the endomyometrium was a depth of 5.4. Late changes showed areas of hyalinization and the presence of basal endometrium (35). Vilos et al. (36) did a study using a latex balloon and involved 30 patients. All patients were discharged within 4 hours. No improvement was seen in 17% at 3 months, 17% at 6 months, and 23% at 12-18 months. A hysteroscopic examination was done immediately following treatment. Under hysteroscopic visualization, a uniformly blanched fundus, anterior wall, and sidewalls were observed. A pink area of 5-10 mm diameter was seen around the tubal ostea as well as the posterior uterine wall in retroverted uteri, implying that energy distribution was not uniform. More uniform blanching may be achieved if the fluid was constantly agitated in the balloon. Vilos et al. (37) studied 121 women with serious menorrhagia. A balloon was inflated with 5% dextrose and heated to 87 ± 5°C. The diameter of the device was 4.5 mm and length was 16 cm. Most patients required no cervical dilatation. Balloon pressures were between 140-190 mmHg during the thermal treatment. The patients’ menstrual blood loss was measured by comparing their pads pre- and post treatment. The success rate was 86-90%. Analysis of the data correlated increased age of the patient to increased success. An initial pressure of 150 mmHg was required to activate the system. A temperature of 87°C was controlled at the heater surface and an 8 minute treatment was given once the heater reached the target temperature. Shah (38) performed work to study temperature distributions during balloon heating. The study was done in two phases: 1) ex-vivo with 9 uteri and 2 control; and 2) in-vivo with 8 uteri and 1 control, using a latex balloon. Temperature probes were placed in the serosa, myometrium, and endometrium piror to heating. The probes in the endometrium were pulled back slightly so as not to puncture the balloon, so the resulting temperatures will underestimate the endometrial surface temperature. All treatments were for an 8 minute duration, except for one uterus which was given a 24 minute treatment. Results are shown in Table 1. TABLE 1
The depth of damage was determined histologically. For the ex-vivo experiments, the deepest single depth was 5.8 mm and the mean myometrial depth of damage was 3.4 ± 1.8 mm. One patient was given three treatments. In the triple treatment specimen, the deepest single depth of damage was 7.9 mm. For the in-vivo specimens, the deepest depth of damage was 3.4 mm and the mean depth of damage was not reported, but is assumed to be less. An alternate balloon therapy was given with a larger, 10 mm device that required cervical dilatation. The balloon membrane was silastic and pressure was maintained at 200 mmHg during treatment. The user was required to add volume to the balloon to maintain this pressure during a 15 minute treatment. The balloon also had a stirring mechanism to mix the fluid in the balloon. The temperature of the balloon was measured at the heater location in the center of the balloon and no temperature sensors were in contact with tissue (39). Meyer et al. (40) performed a randomized trial of a latex balloon vs. rollerball ablation. A follow-up with 239 patients was done and results shown in Table 2. No pretreatment was done for endometrial thinning. The depths of the uterine cavities were between 4 and 10 cm. TABLE 2
2.6Microwave ablationPrior et al. (5) described an endometrial ablation device utilizing microwave energy. The treatment consisted of a probe placed in the uterine cavity and capacitively coupled to electrodes on a belt around the patient at 27.12 MHz. An electric field was set up around the active tip of the probe to heat the adjacent endometrium (72). The intrauterine electrode was 10 mm in diameter and 70 mm in active length, although was custom tailored to each patient with a selection of 50, 60 or 70 mm, depending on the uterine cavity length. The active probe was connected to a 200 mm long, nylon rod. The belt around the patient’s abdomen consisted of a wire mesh embedded in an insulating material and placed in the same plane as the probe. The inner layer was a 70 mm wide stainless steel mesh of 0.013 mm wire on a 1.0 mm grid. The microwave signal was applied to the probe source. The electrical load presented was the probe, patient, and external belt matched to the generator output by a tuning circuit to form a series resonant circuit. Once tuned, most of the power was applied to the endometrium. In this system, the heating falls off inversely with distance. In the uterine environment with a rich blood supply, the underlying myometrium acts as a protective heat sink to prevent too much penetration (41). In the high density electric field, ECG electrodes needed to be applied with care and patient-metal contact had to be avoided to prevent radiofrequency bums. Ex-vivo temperature measurements were made on uterine tissue at room temperature. Results at various depths were 35°C (0.0 mm), 30°C (5.0 mm), 20°C (10 mm), and 18°C (20 mm). In their clinical study, patients were treated with a power level of 550 W. The treatment time influenced the success rate with 10, 15 and 20 minute treatments resulting in 30, 60, and 84% success rates, respectively. Some of the patients had lower abdominal cramps for 48 hours. Contact between the probe and the vaginal wall was possible, resulting in two patients having a fistula 3-4 weeks following treatment, that resulted in urinary incontinence. A nylon insulating layer was added to the probe in subsequent treatments to prevent this complication. A study of 1280 women was done with the results showing a 79% patient satisfaction at 6 months following the treatment. The Menostat (Rocket Medical, UK) was used at 27.12 MHz. (42). The slightly curved probe was rotated during the 20 min. treatment. Severe uterine cramping for the next 6 hours was seen, as well as at discharge from the hospital at 8-24 hours. All patients were medically pretreated to thin the endometrium. The disposable applicators had 3 sizes: small, medium and large. Power applied was 50-200 W. Results showed that 16% were dissatisfied and 14% had amenorrhea. Complications included 10 skin bums on buttocks or chest due to the abdominal belt, 3 uterine perforations, 5 vaginal fistulas, 1 thermal injury of the bowel which required partial excision of the bowel and hysterectomy. There was also one case of thermal injury to the cervix. Further studies with this device showed that the temperature at the endometrial surface was 65°C and at 10 mm depth was 40°C. The temperatures were maximum at the endometrial surface. The uterine serosa rose 3°C and the bowel, bladder, and abdomen rose 0°C. Advantages proposed by the technology were that at 27.12 MHz, direct tissue contact was not necessary, due to capacitive coupling. Thus, irregularity of the endometrial cavity did not preclude uniform heating. The total energy delivered was in the range of 330-660 kJ. Lastly, the patients with the highest dose had moderately severe pain afterward (43). More recent studies of this microwave treatment for menorrhagia treated 43 women with 46 treatments. Treatment time averaged 141 s. The result was an amenorrhea rate of 37.2% and an overall satisfaction rate at 3 years of 84% (44). 2.7RF heating with a balloon deviceAn alternate technology utilized an air filled balloon with 12 conductive patches on the outside surface. Each patch had a thermistor for temperature sensing, in contact with tissue. A grounding pad was placed on the patient and RF energy was multiplexed among the patch electrodes such that each was activated individually for a short time. The shaft was 10 mm and required cervical dilatation. When inflated with air, the balloon pressure compressed the endometrium. Due to the edge effects of the electrodes when energized with RF, the gap between the electrodes when the balloon was inflated, heated well with no cool areas. Each electrode was energized in such a way that the temperature at the sensor in contact with tissue was maintained at the setpoint. The target temperatures were 72-75°C, depending on location, and 10 ml of air was used to inflate the balloon. A power level of 40-45 W at 500 kHz was used during the 4 minute treatment. In the study of 69 patients, there were 2% failures at 3 months and 40% amenorrhea rate. Of the patients in the study, 89% experienced improvement. A second study with the same technology was performed on 187 patients. The warm-up period to reach the target temperature was 3 minutes or shorter. Treatment time commenced following warm-up and took place over a period of 4 minutes. The amenorrhea rate was 38% and bleeding was reduced in 95% of the patients. Thermal destruction was 4-5 mm into the myometrium (45, 73) Brooks et al (46) described a disposable elastic balloon covered with an array of electrodes, each with a temperature sensor, and a computerized controller that connected to a standard electrosurgical generator. Temperatures at the tissue-electrode interface were monitored throughout the procedure. A prehysterectomy study in 30 women showed no significant rise in serosal temperature during treatment. The residual endometrium was 0.2 mm and typical depth of necrosis from 2 to 4 mm into the myometrium, measured histochemically with hematoxylin and eosin (H&E) or nitroblue tetrazolium (NBT). Therapeutic procedures were successfully performed with paracervical block and minor intravenous sedation. Thomsen et al. (1) performed a histopathological study comparing three balloon devices on a group of prehysterectomy patients. The devices under study included two hot fluid, conductive heating balloons. One circulated the fluid and one did not. The other device was the RF balloon with individual temperature control. A total of 19 patients were studied, five for each of three balloon devices, as well as sham heating patients where the devices were placed and no heat was applied. Each uterus was sectioned into 24 blocks. Each block represented a transmural section including endometrium, myometrium, and serosa. Thermal damage was assessed in three ways. Sections were stained with NBT (see Figure 3) to demonstrate the presence of vital and respiratory enzymes. The red zone of the fixed samples showed the outer boundary of thermal damage (se Figure 2). Lastly, the clear zone showed the boundary of thermal coagulation and shrinkage on H&E stained tissue sections. The results are shown in Table 3. For more discussion of thermal damage see Thomsen and Pearce (46) and McMurray et al. (47). One patient was treated and then had a hysterectomy four days later. The tissue sample is shown in Figure 1. FIGURE 1Gross pathology of slice of uterine wall after thermal ablation at the endometrial surface 4 days prior to hysterectomy. A balloon device in the uterine interior was used to treat the endometrium to ablate this layer and extend into the myometrium.  FIGURE 2Gross pathology of uterine wall slice after thermal treatment of the endometrium. The zone of damage is indicated by the color change as one travels down from the surface (top of sample). The endometrium layer is at the top.  FIGURE 3Gross pathology of uterine wall slice following thermal endometrial ablation. The sample has been stained with NBT. The light zone is indicative of non-viable tissue.  TABLE 3
Differences among the devices are due to several factors. The multi-electrode balloon treats with 12 individually controlled patches for four minutes. Less very deep and very shallow depth of damage results were seen. The non-circulating balloon treated for 8 minutes to 87°C and the circulating balloon to 76-77°C for 15 minutes. See Thomsen et. al. (1) for histograms showing the distribution of depth of damage among the devices. 2.8CryotherapyCryotherapy has also been used for endometrial ablation to reduce abnormal bleeding. A probe was inserted into the uterus and the freezing initiated, usually with the probe moving slowly side-to-side; or alternately, freezing and then moving to the other side of the uterus and freezing again. Cryocoagulation of the endometrium at the uterine cornua was studied by Droegemueller et al. (48). A cryoprobe was used to produce coagulation necrosis and subsequent scar formation of the cornual areas of the uterus. A development program was elucidated with instrument design, efficacy and safety testing in baboons, as well as preliminary investigations for human use. Rutherford (49) performed a study with a cryoprobe which was maintained at -176°C. Some patients were under general anesthesia and some were given paracervical block only. A pre- and post-operative MRI series was done and the post-operative series showed a decreased endometrial stripe and globular edema in the fundus. A second study by Rutherford et al. (50) was done in 15 patients. Amenorrhea rates of 76% at 6 months and 50% at 22 months were shown. Work by Raczek and Malarewicz (51) showed cryotherapy results on 10 patients, aged 35-45 years. Previously all of them had undergone dilatation and curettage. Pre-operatively, the patients were treated with medroxyprogesterone until the endometrium reached the thickness of 4 mm. A 0.9% saline irrigant was used as an uterine distension medium. There were no operative complications. In the first 24 hour period after the treatment, clear vaginal discharge appeared which lasted no longer than 14 days. The first vaginal ultrasonography 2 months after the treatment showed either lack of, or only traces of endometrium. In all the patients, a small amount of menstrual bleeding appeared in the 7th week following the treatment, and continuing until the 6th month of observation. Another endometrial cryoablation technique was described that used a probe utilizing the Joule-Thompson principle of expanding gases and operated in a saline environment. The Joule-Thompson electrode allowed for a smaller diameter of the treatment device. During treatment, two freeze-thaw cycles were used (52). A prospective study of 67 women was done with. The probe had a channel to inject saline solution into the uterine cavity. The probe was introduced into the uterine cavity, which was distended with 5 ml saline solution. The device was then activated for two freeze-thaw cycles where the saline solution forms an ice mold of the uterine cavity which can be observed on ultrasound. No surgical or long-term complications were observed and two-thirds of the patients followed up for greater than three months were completely satisfied. An improvement in menstrual symptoms was found in 63% of patients followed up for 3-18 months. Rutherford et al. (50) studied cryotherapy and remarked that early endometrial destruction using cryotherapy achieved mixed results, although improvements in technology now allowed more rapid and extensive freezing. A study was preformed on 15 women with MR done within one week of the procedure and at 65 months. Dilatation and curettage was performed prior to the treatment. During the treatment, a probe of 8 mm diameter and 27 cm length was inserted into the uterus until it was in contact with the uterine fundus. The probe had a conical tip with a freezing zone of 4 cm along the distal portion of the device. Within 3-5 minutes of the probe activation, the temperature at the probe reached -170°C and the front of the ice ball was about halfway through the myometrium. The freezing was then discontinued and thawing began. If the endometrial cavity length exceeded 6 cm, the probe was released from the iceball during the first activation and then pulled back to freeze the proximal uterine segment to -20°C. Most of the patients in the study were released the same day. All had a discharge over the next 4-8 weeks. At the end of 6 months, the amenorrhea rate was 75.5%, although this figure dropped to 50.2% at 22 months. 3.NUMERICAL SIMULATIONSIn order to predict temperatures at various time points, a two-dimensional, finite element model was set up. Modeling code was developed (53, 54) and allowed thermal and electrical properties to vary with temperature, time, or location. It simulated both RF devices that deposit power in tissue and purely conductive heating devices. It was based on the bioheat equation (8) as shown in Eq. 1. Simulations were made of endometrial ablation treatment in this finite element model. Both RF or balloon conductive devices were simulated by using the treatment parameters of time and temperature, as in the clinical studies. Thermal conductivity, electrical conductivity, and perfusion were functions of temperature. It has been previously shown that when heating beyond 60°C, the electrical conductivity of tissue changes enough to make a visible difference in the predicted temperature distribution. It has also been shown in clinical trials (55) that as the electrodes heat tissue, electrical conductivity increases and as temperatures begin to stabilize and plateau, so does the conductivity. Electrical conductivity measurements were made (12) after techniques by Wang et al. (56). In addition, thermal conductivity of uterine tissue was analyzed in fresh uterine samples and found to be 0.536 W (m-1) K with 81% water content. Endometrium with myometrium was 0.542 W (m-1) K (57). Thermal properties also vary with temperature, and muscle measurements were made in the laboratory at the University of Colorado (Roop Mahajan, personal communication). Thermal conductivity as a function of temperature was placed in a table for use in the simulation. Two devices were modeled, both based on balloon technologies. The treatment objectives were to heat and ablate the endometrium, the inner lining of the uterus, with a single application of heat in under 15 minutes. The RF system was composed of a balloon with a silastic membrane. The balloon surface had electrodes composed of copper patches, each with a central thermistor in contact with tissue (45, 58). The electrodes were mounted on an air filled membrane which when inflated may lower perfusion in adjacent tissue. RF current was multiplexed among the electrodes (0.5 s on time) which share a common return electrode mounted elsewhere on the body. The thermistors in the center of each electrode were controlled to 72 or 75°C for four minutes, after a one minute heatup. A Dirichlet electric boundary condition with constant voltage was applied at the electrode surfaces. A Nuemann electric boundary condition with zero flux was applied at the outer surfaces of the uterine tissue block, except along the ground. Voltage at the ground was set to 0.0 V. A second case was also simulated where no external ground was used. In this bipolar case, the left and right electrodes were alternatively activated and a voltage applied between them and the center electrode. The second technology utilized a heating source in a dextrose filled balloon. The heat source was temperature-controlled to 87°C and was located in fluid in the center of the balloon. The fluid was not circulated. Treatment time was eight minutes, once the setpoint is reached (32, 33). Simulation results are seen in the following section. The model is 2D and the uterine wall is 2.5 cm. The balloon occupies the lower 1.0 cm and the two closely spaced parallel lines (horizontal) show the location of the insulating silastic or latex layer. Above this layer is the uterine tissue. The perfusion of the uterus is assumed to be greater than muscle. The first simulations in Figures 4-11 are for the case of the balloon with the conductive patches on the outside, in contact with tissue. The balloon is air filled. Figures 4-7 represent the case where there are three electrodes at locations 1.2 to 2.0, 2.6 to 3.4, and 4.0 to 4.8 mm, along the x-axis above the insulating layer. Ground is the upper portion of the block model. The lines of constant electric field are seen in Figure 4 and the power density in Figure 5. Since the electrodes are multiplexed, only the left electrode is on at this time. Current lines will be perpendicular to the lines of constant electric field and the current value will be proportional to the closeness between lines. The power density plot shows the effects of the electrode edges, which concentrate power, and also the effect of the presence of the adjacent (center) electrode. FIGURE 4The figure shows lines of constant electric field for three electrodes mounted on an air-filled, silastic balloon in uterine tissue. The electrodes are multiplexed and ground is the top surface. Only the left electrode is energized.  FIGURE 5The figure shows power density for an RF balloon with three electrodes which are time multiplexed. The left electrode is energized.  The bioheat equation predicts the isotherm distribution as seen in Figure 6, the results at one minute. At this point the heat up should be complete and the treatment time of 4 minutes commences. The left and right electrodes are given an initial voltage of 53.9 V to achieve a 72°C target in 60 s. The center electrode is given an initial voltage of 43.3 V to achieve a 75°C target in 60 s. Once this state is achieved, the treatment phase begins. The applied voltages for this phase were 23.5 V (left and right) and 9.0 V (center). Figure 6 shows the temperature snapshot at the end of the heatup phase. Some temperatures exceed 100°C in the gap between the electrodes. The gap is assumed to be 6 mm in the distended balloon, which is realistic for the clinical device. Figure 7 shows the isotherms at the end of treatment when thermal conduction has smeared the temperature gradients. FIGURE 6The figure shows isotherms for three electrodes mounted on an air-filled, silastic balloon in uterine tissue activated with RF monopolar energy. The electrodes are multiplexed and ground is the top surface. The results are for the end of heatup at 1 minute.  FIGURE 7The figure shows isotherms for three electrodes mounted on an air-filled, silastic balloon in uterine tissue activated with RF monopolar energy. The electrodes are multiplexed and ground is the top surface. The results are for the end of treatment at 4 minutes.  The second RF balloon case is for the same three electrodes as the first case, except that the electrodes are now run in a bipolar configuration. The system is multiplexed between the left and center electrodes for 0.5 s and then the right and center electrodes are activated. Now only two control voltages are applied, unlike the first case when all three electrodes were independent. Now all current flows between adjacent electrodes, although the presence of a conductive electrode in the proximity of the other two has an effect on the electrode field as seen in Figure 8. The power density with the left/center combination on is seen in Figure 9. Most power is in the gap and at the electrode edges. FIGURE 8The figure shows lines of constant electric field for three electrodes mounted on an air-filled, silastic balloon in uterine tissue. The electrodes are operated in a bipolar fashion with a voltage applied to either side electrode relative to the center electrode.  FIGURE 9The figure shows the results of power deposition for a three electrode case on an air filled balloon. A bipolar configuration is used between left and center electrodes.  The results of the bioheat equation are shown in Figures 10 and 11, respectively, for 1 minute of heatup and 4 minutes of treatment. Figure 10 shows temperatures exceeding 120°C and Figure 11, exceeding 100°C. Initial voltages applied are 70.0 V between left or right and the center. For steady-state treatment, a voltage of 27.2 V is applied. FIGURE 10The figure shows isotherms for three electrodes mounted on an air-filled, silastic balloon in uterine tissue. The electrodes are operated in a bipolar fashion with a voltage applied to either side electrode relative to the center electrode. The results are for the end of heatup at 1 minute.  FIGURE 11The figure shows isotherms for three electrodes mounted on an air-filled, silastic balloon in uterine tissue. The electrodes are operated in a bipolar fashion with a voltage applied to either side electrode relative to the center electrode. The results are for the end of treatment at 4 minutes.  The hot fluid cases are seen in Figures 12 and 13. In Figure 12, an 87°C heater is in dextrose and after a 1 minute heatup, an 8 minute treatment is given. Thermal gradients are still persistent at the end of the treatment. If we mix the fluid in the dextrose, lower the temperature to 76°C, and extend the treatment time to 15 minutes, the results are seen in Figure 13. Some heat is lost across the latex barrier, shown as the closely spaced parallel lines at y=l cm. FIGURE 12The figure shows isotherms for the results of a non-circulating balloon device, filled with fluid. The source temperature is 87°C and no mixing of the fluid is assumed due to patient movement or respiration. The time is at the end of treatment at 8 minutes. 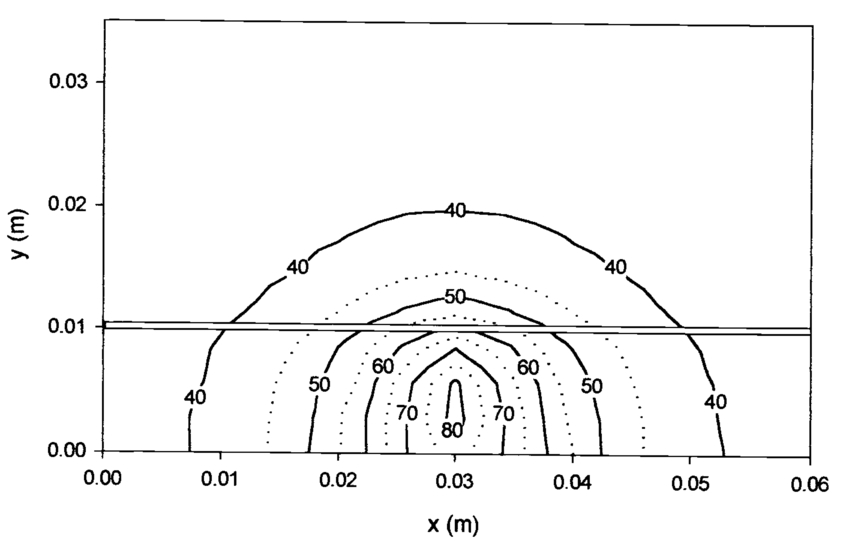 FIGURE 13The figure shows the results of a temperature distribution calculated for a fluid-filled balloon at 15 minutes, with the assumption that the fluid circulates and is controlled at 76°C.  Figure 14 shows the heatup at the center of the three electrodes when activated in the monopolar, multiplexed RF scheme (from Figures 4-7). The left and right electrodes have a 72°C target and the center electrode target is 75°C. Measurements in the simulation were made at the electrode center in contact with tissue, mimicking clinical cases. Figure 15 is for the bipolar RF case (from Figures 8-11). The center electrode is now uncontrolled and reaches 105°C during heatup.
FIGURE 14Plot of temperatures at center of electrodes in contact with tissue. Monopolar RF electrodes are multiplexed. A 60 s heatup is followed by a 4 minute treatment.  FIGURE 15Plot of temperatures in a bipolar RF system with the outer electrodes held at 75°C. The outer electrodes are multiplexed with the center electrode in a bipolar fashion. A 60 s heatup is followed by a 4 minute treatment.  The following assumptions were made in the model: 5.DISCUSSIONAbout 10-20% of the hysterectomies done annually in the US are due to abnormal uterine bleeding, although hysterectomy is no longer an acceptable alternative for many women. In response to the quest for alternative treatments, surgical procedures that utilize rollerball ablation or loop resection have become popular and the “gold standard”. Since both of these procedures operate in a non-conductive fluid environment and utilize tools with a potential to cut and bum through tissue, the morbidity is higher than practitioners would prefer. A number of studies reported a range of complications from rollerball or loop resection of the endometrium, including severe hemorrhage from uterine or internal iliac vessels, uterine perforation, bowel and ureter damage, excessive fluid absorption, gas embolus, and sometimes death from these complications (21, 59). These early surgical ablation methods had the advantage of short hospital stay, reduction of bleeding, rapid recovery, and most importantly, retention of the uterus. Alternatives were long-term medication, hysterectomy, and Nd:YAG laser ablation, used since the 1970s. These procedures are not a minor surgery and require a skilled surgeon (21). Complications of surgical ablation include fluid overload and perforation. Due to the potential morbidity, an argument can be made for a safer alternative where user skill and fluid uptake are no longer issues. Dilatation and curettage was an early solution to abnormal bleeding and although may bring some relief, the durability is only a few menstrual cycles. The thermal balloon therapy is the safest of the treatment options (61). Simple devices inserted transcervically and computer controlled and monitored provide viable alternatives to a surgical procedure. In addition, fifty percent of specimens obtained at hysterectomy for menorrhagia are free of disease and thus lacking organic pathology. This argues for a treatment to solve the abnormal bleeding problem, not surgery (38). The vascular supply of the endometrium resides deeper in the underlying myometrium and best results are obtained when the superficial myometrium is also damaged (25). There are still some considerations regarding patient satisfaction with the thermal treatments available. Unlike hysterectomy which eliminates all bleeding, the thermal treatments reduce bleeding substantially in about 80-90% of cases. The amenorrhea rate is not as high. Some women regard bleeding at any level as a disappointment after this procedure. Other studies argue that residual endometrium in the cervical os may recolonize either partially or totally, the ablated uterine cavity. They further argue that women may dislike amenorrhea since they will now lack the proof of not being pregnant (24). After thermal destruction of the endometrium, a viable surface that will nurture pregnancies is no longer available. One study reported that there were three pregnancies after the ablation procedure. Of these, two had abortions and one proceeded to 28 weeks, then experienced intrauterine death. This was likely due to poor placental development due to the sparse endometrium. It was suggested that women undergoing endometrial resection of ablation should practice birth control (17). Tresserra et al. (62) did thermal ablation and with some of the treatment failures performed a hysterectomy. Tissue was harvested during the surgery at 19 ± 17 months. Scarring with formation of additional endometrial cavities was seen in 5/12 and cervical stenosis was seen in 2/12 cases. Necrosis was present in some cases. Adenomyosis was seen in 6/7 cases where the endometrium had regenerated and probably led to treatment failure. There are a range of methods and device types available or currently in clinical trials. Lewis (63) has shown that if a probe was used that relied strictly on conductive heating with the aim to achieve an endometrial temperature in excess of 50°C, the probe would have to exceed 100°C. Instead, his group developed a device operational at 27.12 MHz, with a lkW amplifier and a tuning unit. In a typical treatment which lasted 12-15 minutes, the probe surface achieved a temperature of 60-65°C. This device with its large belt around the patient may cause undiscovered heating at a considerable distance from the probe. A strict protocol was required that dictated patient position, general anesthesia, drained bladder, and no alcohol products used in the patient preparation due to flammability concerns. The organ at greatest risk was the bladder. One patient had a bum on the finger due to the pulse oximeter attachment. In the work presented here, different depths of damage as well as shape of the damaged region are shown. The 55°C isotherm is assumed to be the boundary of damage. In the RF monopolar balloon case, the depth of damage was 11.3 mm and in the bipolar case, 7.5 mm, as seen fin Figures 7 and 11 respectively. In the conductive balloon cases, the depths of damage were 1.0 and 4.7 mm, respectively for the non-mixing and the mixing cases, respectively, seen in Figures 11 and 12. The shape of the heating zone for the mixing balloon is more uniform than the RF cases. The assumptions in the non-mixing balloon which show the minimum value of thermal damage probably underestimate thermal damage due to patient muscular movement and respiratory movement during treatment which would tend to mix the fluid. The model assumes no mixing. Jain and Wolf (60) compared lesioning at constant power versus temperature control. With temperature control, the lesion growth was fastest during the first 20 s and slowed and became steady-state after 100 s. In constant power mode, the lesion growth was also fastest during the first 20 s, although did not reach steady state even after 600 s. The electrical conductivity of the tissue that changes with temperature is responsible for the continuous lesion growth. Positioning of the ground in their monopolar model affected lesion size. This work does model a change in electrical conductivity with temperature and so should compensate for lesion size changes due to the changing properties. There are reasons that many devices are temperature-controlled rather than placed in a constant power mode. If temperatures are excessive and reach values higher than 110-120°C, steam formation and popping and mechanical damage may ensue (60). In addition, if tissue chars excessively, it may adhere to the device and thus be difficult to remove. The finite element model in this paper produced simulations that helped predict clinical heating depths. Since when heating beyond 60°C the electrical conductivity of tissue changes enough to make a difference in the predicted temperature distribution, the values as a function of temperature were input into the simulations. Thus, a versatile model should have the capability of inputting changing tissue parameters when temperatures are high enough to affect results and thus will better predict tissue thermal events in biological systems. If the heat flux is very large and the time duration is very small, the change in perfusion with temperature is not as significant (64). This is definitely not the case when heating over a 4-15 minute time period. Thermal doses of time and temperature affect various tissues differently (66, 67, 68, 69), however, and depending on the temperature level, the tissue could be irreversibly altered. These results agree with work at lower frequencies (65) that demonstrated the effects of irreversible damage (70). In the uterine model, the wall thickness is 2.5 cm which is representative of human uterus and gives a margin of safety when heating 5-10 mm into the tissue. Thus, a model which incorporates changing electrical, thermal and perfusion properties of tissue as a function of temperature is required In both the RF and conductive heating designs, the simulations are useful in designing the dimensions of the products. In the conductive heating system, the model will help predict the extent of thermal damage if the time or control temperature is changed. If the balloon thickness or material is changed, the model can show the differences in outcome. If the tissue is pathological and has different thermal properties or perfusion, these can be input into the simulation. For the RF balloon, the model can assist in optimizing the size and spacing of the electrodes, choosing the conductive and insulating materials and thicknesses, choosing air or fluid for filling a balloon, choosing the temperature setting based on the tissue temperature, thermal sensor location, identification of hot and cold spots, and determination of optimal treatment time. In addition, comparison between a bipolar system when current flows between electrodes or a monopolar system where electrodes are multiplexed or are simultaneously activated can be investigated. A number of new devices are currently being studies and are in FDA review. These include novel bipolar RF and cryotherapy techniques. As in all the treatment regimes, the durability of the treatment must be carefully studied in long-term follow-up. 6.ACKNOWLEDGMENTSDr. Sharon Thomsen was the thermal damage expert who contributed to this publication. 7.7.REFERENCESS.L. Thompsen, T. Ryan, K. Kuk-Nagel, C. Soto, T.G. Vancaillie, and J. Garza-Leal,
“Quantitative and qualitative histopathological comparisons of multielectrode balloon and thermal balloon endometrial ablation,”
in SPIE,
115
–124
(1998). https://doi.org/10.1117/12.304335 Google Scholar
R. Hurskainen, J. Teperi, J. Paavonen, and B. Cacciatore,
“Menorrhagia and uterine artery blood flow,”
Hum. Reprod., 14 186
–189
(1999). https://doi.org/10.1093/humrep/14.1.186 Google Scholar
A.A. Shah, and D.A. Grainger,
“Contemporary concepts in managing menorrhagia,”
Medscape Womens Health, 1 8
(1996). Google Scholar
H.A. Goldfarb,
“A review of 35 endometrial ablations using the Nd:YAG laser for recurrent metromenorrhagia,”
Obstet. Gynecol., 76 833
–835
(1990). https://doi.org/10.1097/00006250-199011000-00022 Google Scholar
M.V. Prior, J.H. Phipps, T. Roberts, B.V. Lewis, J.W. Hand, and S.B. Field,
“Treatment of menorrhagia by radiofrequency heating,”
Int. J. Hyperthermia, 7 213
–220
(1991). https://doi.org/10.3109/02656739109004991 Google Scholar
F. Nagele, T. Rubinger, and A. Magos,
“Why do women choose endometrial ablation rather than hysterectomy?,”
Fertil. Steril., 69 1063
–1066
(1998). https://doi.org/10.1016/S0015-0282(98)00082-X Google Scholar
I.S. Fraser, D.L. Healey, H. Torode, J.Y. Song, P. Mamers, and F. Wilde,
“Depot Goserelin and Danazol pre-treatment before rollerball endometrial ablation for menorrhagia,”
Obstet. Gynecol., 87 544
–550
(1996). https://doi.org/10.1016/0029-7844(95)00475-0 Google Scholar
H.H. Pennes,
“Analysis of tissue and arterial blood temperatures in the resting human forearm,”
J. Appl. Physiol., 1 93
–122
(1948). https://doi.org/10.1152/jappl.1948.1.2.93 Google Scholar
J.W. Strohbehn,
“Temperature distributions from interstitial RF electrode hypothermia systems: theoretical predictions,”
Int. J. Rad. Oncol. Biol. Phys., 9 1655
–1667
(1983). https://doi.org/10.1016/0360-3016(83)90419-4 Google Scholar
K.D. Paulsen, X. Jia, and J.M. Sullivan,
“Finite element computations of specific absorption rates in anatomically conforming full-body models for hyperthermia treatment analysis,”
IEEE Trans. Biomed Engin., 40 933
–945
(1993). https://doi.org/10.1109/10.245615 Google Scholar
J.A. Mechling, and J.W. Strohbehn,
“Three-dimensional theoretical SAR and temperature distributions created in brain tissue by 915 and 2450 MHz dipole antennas with varying insertion depths,”
Int. J. Hyperthermia, 8 529
–542
(1992). https://doi.org/10.3109/02656739209037990 Google Scholar
J.S. Dadd, T.P. Ryan, and R.C. Platt,
“Tissue impedance as a function of temperature and time,”
Biomed. Scien. Instrum., 32 205
–214
(1996). Google Scholar
H. P. Schwan, and K.R. Foster,
“RF-field interactions with biological systems: electrical properties and biophysical mechanisms,”
in Proc. IEEE,
104
–113
(1980). Google Scholar
S. Labonte,
“Numerical model for radio-frequency ablation of the endocardium and its experimental validation,”
IEEE Trans. Biomed. Engin., 41 108
–115
(1994). https://doi.org/10.1109/10.284921 Google Scholar
P.A. Patel, J.W. Valvano, J.A. Pearce, S.A. Prahl, and C.R. Denham,
“A self-heated thermistor technique to measure effective thermal properties from the tissue surface,”
Trans. ASME, 109 330
–335
(1987). Google Scholar
P.G. Brooks, and S.P. Serden,
“Endometrial ablation in women with abnormal uterine bleeding aged fifty and over,”
J. Reprod. Med., 37 682
–684
(1992). Google Scholar
S.C. Nicholson, R.J. Slade, A.I.H. Ahmed, M.D.G. Gillmer,
“Endometrial resection at Oxford: the first 500 cases,”
Obstet. Gynaecol., 15 38
–43
(1995). https://doi.org/10.3109/01443619509007733 Google Scholar
T.G. Vancaillie,
“Electrocoagulation of the endometrium with a ball-end resectoscope,”
Obstet. Gynecol., 74 425
–427
(1989). Google Scholar
J.P. Van Damme,
“One-stage endometrial ablation: results of200 cases,”
Eur. J. Obstet. Gynecol. Reprod. Biol., 43 209
–214
(1992). https://doi.org/10.1016/0028-2243(92)90175-X Google Scholar
J.F. Daniell, B.R. Kurtz, and R.W. Ke,
“Hysteroscopic endometrial ablation using the rollerball electrode,”
Obstet. Gynecol., 80 329
–332
(1992). Google Scholar
I.S. Fraser, S. Angsuwathana, I. Mahmoud, and S. Yezerski,
“Short and medium term outcomes after rollerball endometrial ablation for menorrhagia,”
Med. J. Austral., 158 454
–457
(1993). Google Scholar
P.D. Indman, and R.M. Soderstrom,
“Depth of endometrial coagulation with the urologic resectoscope,”
J. Reprod Med., 35 633
–635
(1990). Google Scholar
H. Moseley, M.M. Glegg, M.J. Evans, S. Ellis, and L.J. Grant,
“Stray RF field strength during radiofrequency endometrial ablation,”
J. Med Eng. Technol., 20 127
–133
(1996). https://doi.org/10.3109/03091909609008391 Google Scholar
P. Vercellini, S. Oldani, L. Yaylayan, B. Zaina, O. DeGiorgi, and P.G. Crosignani,
“Randomized comparison of vaporizing electrode and cutting loop for endometrial ablation,”
Obstet. Gynecol., 94 521
–527
(1999). Google Scholar
M. Baggish, M. Paraiso, E.M. Breznock, and S. Griffey,
“A computer controlled, continuously circulating, hot irrigating system for endometrial ablation,”
Am. J. Obstet. Gynecol., 173 1842
–1848
(1995). https://doi.org/10.1016/0002-9378(95)90438-7 Google Scholar
J. Donnez, R. Polet, P.E. Mathhhieu, E. Konwitz, and M. Nisolle,
“Endometrial laser interstitial hyperthermy: a potential modality for endometrial ablation,”
Obstet. Gynecol., 87 459
–464
(1996). https://doi.org/10.1016/0029-7844(95)00412-2 Google Scholar
R.B. Everett,
“Five year review of endometrial ablation with the sidefire laser fiber,”
J. Am. Assoc. Gynecol. Laparosc., 6 65
–69
(1999). https://doi.org/10.1016/S1074-3804(99)80043-7 Google Scholar
M.S. Baggish, and E.H.M. Sze,
“Endometrial ablation: a review of 568 patients treated over an 11-year period,”
Am. J. Obstet. Gynecol., 174 908
–913
(1996). https://doi.org/10.1016/S0002-9378(96)70324-1 Google Scholar
R. Phillips,
“Endometrial ablation for postmenopausal uterine bleeding induced by hormone replacement therapy,”
J. Am. Assoc. Gynecol. Laparosc., 2 389
–393
(1995). https://doi.org/10.1016/S1074-3804(05)80058-1 Google Scholar
V.L. Baker, and G.P. Adamson,
“Intrauterine pressure and uterine distension,”
J. Am. Assoc. Gynecol. Laparoscop., S3 3
(1996). https://doi.org/10.1016/S1074-3804(96)80135-6 Google Scholar
Singer, R. Almanza, A. Gutierrez, G. Haber, L.R. Bolduc, and R. Neuwirth,
“Preliminary clinical experience with a thermal balloon endometrial ablation method to treat menorrhagia,”
Obstet. Gynecol., 83 732
–734
(1994). Google Scholar
R.S. Neuwirth, A.A. Duran, A. Singer, R. Macdonald, and L. Bolduc,
“The endometrial ablator: anew instrument,”
Obstet. Gynecol., 83 792
–796
(1994). Google Scholar
M.B. Fortin, and B. McColl,
“Gynecare UBT system under local anesthesia,”
J. Am. Assoc. Gynecol. Laparosc., 3
(S13),
(1996). Google Scholar
N.N. Amso, S.A. Stabinsky, P. McFaul, B. Blanc, L. Pendley, and R. Neuwirth,
“Uterine thermal balloon therapy for the treatment of menorrhagia: the first 300 patients from a multi-center study,”
Br. J. Obstet. Gynecol., 105 517
–523
(1998). https://doi.org/10.1111/bjo.1998.105.issue-5 Google Scholar
K. Banerjee, K. Buckshee, N. Bhatla, and S.D. Gupta,
“Thermal balloon endometrial ablator: a preclinical safety and effectiveness study,”
J. Obstet. Gynaecol. Res., 25 143
–146
(1999). https://doi.org/10.1111/jog.1999.25.issue-2 Google Scholar
G.A. Vilos, E.C. Vilos, and L. Pendley,
“Endometrial ablation with a thermal balloon for the treatment of menorrhagia,”
J. Am. Assoc. Gynecol. Laparosco., 3 3873
–387
(1996). https://doi.org/10.1016/S1074-3804(96)80068-5 Google Scholar
G.A. Vilos, C.A. Fortin, B. Sanders, L. Pendley, and S.A. Stabinsky,
“Clinical trial of the uterine thermal balloon for treatment of menorrhagia,”
J. Am. Assoc. Gynecol. Laparosc., 4 559
–565
(1997). https://doi.org/10.1016/S1074-3804(05)80089-1 Google Scholar
A.A. Shah, S.A. Stabinsky, T. Klusak, K.R. Bradley, J.F. Steege, and D.A. Grainger,
“Measurement of serosal temperatures and depth of thermal injury generated by thermal balloon endometrial ablation in ex vivo and in vivo models,”
Fertil. Steril., 70 692
–697
(1998). https://doi.org/10.1016/S0015-0282(98)00245-3 Google Scholar
C. Friberg, C. Joergensen, and M. Ahlgren,
“Endometrial thermal coagulation—degree of uterine fibrosis predicts treatment outcome,”
Gynecol. Obstet. Invest., 45 54
–57
(1998). https://doi.org/10.1159/000009925 Google Scholar
W.R. Meyer, B. W. Walsh, D.A. Grainger, L.M. Peacock, F.D. Loffer, and J.F. Steege,
“Thermal balloon and rollerball ablation to treat menorrhagia: a multicenter comparison,”
Obstet. Gynecol., 92 98
–103
(1998). https://doi.org/10.1016/S0029-7844(98)00141-0 Google Scholar
J.H. Phipps, B.V. Lewis, M.V. Prior, and T. Roberts,
“Experimental and clinical studies with radiofrequency induced thermal endometrial ablation for functional menorrhagia,”
Obstet. Gynecol., 76 876
–881
(1990). https://doi.org/10.1097/00006250-199011000-00032 Google Scholar
R.F. Thijssen,
“Radiofrequency induced endometrial ablation: an update,”
Br. J. Obstet. Gynecol., 104 608
–613
(1997). https://doi.org/10.1111/bjo.1997.104.issue-5 Google Scholar
J.H. Phipps, B.V. Lewis, T. Roberts, M.V. Prior, J.W. Hand, M. Elder, and S.B. Field,
“Treatment of functional menorrhagia by radiofrequency-induced thermal endometrial ablation,”
Lancet, 335 374
–376
(1990). https://doi.org/10.1016/0140-6736(90)90207-L Google Scholar
D.A. Hodgson, I.B. Feldberg, N. Sharp, N. Cronin, M. Evans, and L. Hirschowitz,
“Microwave endometrial ablation: development, clinical trials and outcomes at three years,”
Br. J. Obstet. Gynaecol., 106 684
–694
(1999). https://doi.org/10.1111/bjo.1999.106.issue-7 Google Scholar
J.H. Dequesne, A. Gallinat, J.G. Garza-Leal, C.J. Sutton, H.F. van der Pas, K. Wamsteker, and J.G. Chandler,
“Thermoregulated radiofrequency endometrial ablation,”
Int. J. Fertil. Womens Med., 42 311
–318
(1997). Google Scholar
S. Thomsen, J.A. Pearce, and W.F. Cheong,
“Changes in birefringence as markers of thermal damage in tissue,”
IEEE Trans. Biomed Engin., 36 1174
–1179
(1989). https://doi.org/10.1109/10.42111 Google Scholar
P.G. Brooks, T. Vancaillie, S.L. Corson, R.M. Soderstrom, P.D. Indman, J. Liu, D. Harrison, J.G. Garza-Leal, J.L. Iglesias-Benavides, C.J. Sutton, A. Gallinat, J. Dequesne, K. Wamsteker, L. Mencaglia, and H. Van der Pas,
“Tissue effects of the vestablate office-based endometrial ablation system,”
J. Am. Assoc. Gynecol. Laparosc., 2
(S65),
(1995). Google Scholar
T. McMurray, and J.A. Pearce,
“Thermal damage quantification utilizing tissue birefringence color image analysis,”
ISA, 8856 235
–242
(1993). Google Scholar
W. Droegemueller, B.E. Greer, J.R.Davis, E.L. Makowski, M. Chvapil, and A. Pollard,
“Cryocoagulation of the endometrium at the uterine cornua,”
Am. J. Obstet. Gynecol., 131 1
–9
(1978). https://doi.org/10.1016/0002-9378(78)90466-0 Google Scholar
T.J. Rutherford,
“Cryosurgery is a simple modality for endometrial ablation,”
J. Am. Assoc. Gynecol. Laparosc., 3 S44
–345
(1996). https://doi.org/10.1016/S1074-3804(96)80287-8 Google Scholar
T.J. Rutherford, T.G. Zreik, R.N. Troiano, S.F. Palter, and D.L. Olive,
“Endometrial cryoablation, a minimally invasive procedure for abnormal uterine bleeding,”
J. Am. Assoc. Gynecol. Laparosc., 5 23
–28
(1998). https://doi.org/10.1016/S1074-3804(98)80006-6 Google Scholar
M. Raczek; and A. Malarewicz A,
“Oddzialu Polozniczo-Ginekologicznego Szpitala Miejskiego w Kielcach,”
Ginekol. Pol., 69 594
–547
(1998). Google Scholar
R. Pittrof, S. Majid, and A. Murray,
“A Transcervical endometrial cryoablation (ECA) for menorrhagia,”
Int. J. Gynaecol. Obstet., 47 135
–140
(1994). https://doi.org/10.1016/0020-7292(94)90353-0 Google Scholar
S. Humphries, R.C. Platt, and T.P. Ryan,
“Finite-element codes to model electrical heating and non-linear transport in biological media,”
Adv. Heat Mass Trans. Biotechnol., 37 131
–134
(1997). Google Scholar
T.P. Ryan, R.C. Platt, J.S. Dadd, and S. Humphries,
“Tissue electrical properties as a function of thermal dose for use in a finite element model,”
Adv. Heat Mass Trans. Biotechnol., 37 167
–171
(1997). Google Scholar
T.P. Ryan, J. Garza-Leal, S. Thomsen, J. Iglasias-Benavidas, T.G. Vancaillie, O. Vidal, and K. Lawes,
“Comparison of thermal and multielectrode balloons for endometrial ablation,”
in Annual meeting of the American Association of Gynecologic Laparoscopists,
(1997). Google Scholar
Y. Wang, P.H. Schimpf, D.R. Haynor, and Y. Kim,
“Geometric effects on resistivity measurements wht four-electrode probes in isotropic and anisotropic tissues,”
IEEE Trans. Biomed. Engin., 45 877
–884
(1998). https://doi.org/10.1109/10.686795 Google Scholar
J. Olsrud, B. Friberg, M. Ahlgren, and B.R. Persson,
“Thermal conductivity of uterine tissue in vitro,”
Phys. Med. Biol., 43 2397
–2406
(1998). https://doi.org/10.1088/0031-9155/43/8/030 Google Scholar
R.M. Soderstrom, P.G. Brooks, S.L. Corson, J. Desquesne, A. Gallinat, J.G. Garza-Leal, J.L. Iglesias-Benavides, P.D. Indman, J. Liu, H. van der Pas, R.A. Stem, C. Sutton, T.G. Vancaillie, and K. Wamsteker,
“Endometrial ablation using a dispensable multi-electrode balloon,”
J. Am. Assoc. Gynecol. Laparosc., 3 403
–407
(1996). https://doi.org/10.1016/S1074-3804(96)80071-5 Google Scholar
V.J. Page,
“Anaesthesia and radiofrequency endometrial ablation,”
Eur. J. Anaesthesiol., 10 25
–26
(1993). Google Scholar
M.K. Jain, and P.D. Wolf,
“Temperature controlled and constant-power radio-frequency ablation: what afects lesion growth,”
IEEE Trans. Biomed. Engin., 46 1405
–1412
(1999). https://doi.org/10.1109/10.804568 Google Scholar
C. Barrow,
“Balloon endometrial ablation as a safe alternative to hysterectomy,”
A.O.R.N. J., 70 83
–90
(1999). Google Scholar
F. Tresserra, P. Grases, A. Ubeda, N.M.A. Pascual, P.J. Grases, and R. Labastida,
“Morphological changes in hysterectomies after endometrial ablation,”
Hum. Reprod., 14 1473
–1477
(1999). https://doi.org/10.1093/humrep/14.6.1473 Google Scholar
B.V. Lewis,
“Radiofrequency induced endometrial ablation,”
Baliere’s Clinical Onstet. Gynaecol., 9 347
–355
(1995). https://doi.org/10.1016/S0950-3552(05)80043-4 Google Scholar
J. Liu, X. Chen, and L.X. Xu,
“New thermal wave aspects on bum evaluation of skin subjected to instantaneous heating,”
IEEE Trans. Biomed Engin., 46 420
–428
(1999). https://doi.org/10.1109/10.752939 Google Scholar
M.J. Moskowitz, T.P. Ryan, K.D. Paulsen, and S.E. Mitchel,
“Clinical implementation of electrical impedance tomography with hyperthermia,”
Int. J. Hyperthermia, 11 141
–149
(1995). https://doi.org/10.3109/02656739509022452 Google Scholar
S.A. Saparetto and W.C. Dewey,
“Thermal dose determination in cancer therapy,”
Int. J. Rad. Oncol. Biol. Phys., 10 787
–800
(1984). https://doi.org/10.1016/0360-3016(84)90379-1 Google Scholar
K.R. Diller, and T.P. Ryan,
“Heat Transfer in Living Systems: Current Opportunities,”
J. Heat Trans., 120 810
–829
(1998). https://doi.org/10.1115/1.2825901 Google Scholar
T.P. Ryan,
“Methods of thermal modelling and their impact on interstitial hyperthermia treatment planning,”
Medical Radiology-Diagnostic Imaging and Radiation Oncology: Interstitial and Intracavitary Thermo-Radiotherapy, 95
–116 Springer-Verlag, Berlin
(1993). Google Scholar
L.M. Lim, A. Patel, T.P. Ryan, P.L. Stranahan, and G.J. Fuchs,
“Quantitative assessment of variables that influence soft-tissue electrovaporization in a fluid environment,”
Urol., 49 851
–856
(1997). https://doi.org/10.1016/S0090-4295(97)00092-7 Google Scholar
F.C. Henriques,
“Studies of thermal injury,”
Arch. Path., 5 489
–502
(1947). Google Scholar
A.E. Bent, and D.R. Ostergard,
“Endometrial ablation with the Neodynium:YAG laser,”
Obstet. Gynecol., 75 923
–925
(1990). Google Scholar
D.A. Hodgson, I.B. Feldberg, N. Sharp, N. Cronin, M. Evans, and L. Hirschowitz,
“Microwave endometrial ablation: development, clinical trials and outcomes at three years,”
Br. J. Obstet. Gynaecol., 106 684
–694
(1999). https://doi.org/10.1111/bjo.1999.106.issue-7 Google Scholar
|




